Physicians are pressured to both serve patients and keep up with the demands of an evolving healthcare system. Keeping yourself in the right frame of mind, while maintaining productivity, is essential to providing excellent care, and maintaining a profitable practice. Here are key ways to assess your stress level, and how to keep your workload, and life responsibilities, manageable.
WHAT IS STRESS?
One of your staff just called in sick. Your first patient is 20 minutes late. The electricity just went out, and the electric company does not know when it will be restored. An angry patient just walked through your front door wondering out loud where her glasses are and why did your staff not call to let her know that they would be late. Your stress levels are just about maxed out.
So, what is stress? Here’s a definition:“Stress is defined as an organism’s total response to environmental demands or pressures. When stress was first studied in the 1950s, the term was used to denote both the causes and the experienced effects of these pressures. More recently, however, the word “stressor” has been used for the stimulus that provokes a stress response. One recurrent disagreement among researchers concerns the definition of stress in humans. Is it primarily an external response that can be measured by changes in glandular secretions, skin reactions, and other physical functions, or is it an internal interpretation of, or reaction to, a stressor; or is it both?”
Stress is part of life. Some stress is good, most stress is bad – especially chronic stress. We all respond to stress in different ways. Because of the variability in types and causes of stress, scientists have had a difficult time agreeing on definitions and even measurement tools. Very few of the measurement tools for stress have been validated.
We found an interesting web site that makes a good effort at measuring stress. This web site gives multiple stress measurement tools. We’ll just highlight two of them. The 360 Assessment looks at lifestyle, occupation, attitude and diet to determine overall stress, then provides tips and resources based on your score. The AIS Workplace Stress Survey serves as a simple screening measure determining the need for further investigation with more comprehensive assessments.
Once you’ve identified that you have stress that is negatively impacting your life, then you need to positively manage the stress. Here are 15 scientifically backed ways to de-stress. You can read more about each of these techniques, and more, by going to the article.
1. Go for a 10 minute walk.
2. Breathe deeply.
3. Use the power of “guided imagery” to elicit a relaxation response.
4. Eat a healthy snack
5. Buy yourself a plant.
6. Step away from the screen.
7. Kiss someone.
8. Turn off your phone.
9. Put on some music.
10. Use a web-based stress management program.
11. Chew gum.
12. Watch a viral video.
13. Use progressive muscle relaxation.
14. Spend time with your best friend.
15. Eat a banana.
Everyone has different ways to deal with stress. If your way is not working, then try something new from the list above.

MARK WRIGHT, OD, FCOVD
Dr. Wright is the founding partner of a nine-partner, three-location full-scope optometric practice. As CEO of Pathways to Success, an internet-based practice management firm, he works with practices of all sizes. He is faculty coordinator for Ohio State’s leading practice management program.

CAROLE BURNS, OD, FCOVD
Dr. Burns is the senior partner of a nine-doctor full-scope optometric practice that she built with her husband, Dr. Wright. She is also the COO of a state-wide nursing care optometry practice. Dr. Burns lectures nationally on practice management and staffing issues. Dr. Burns authored the Specialty Practice section of the textbook, Business Aspects of Optometry.













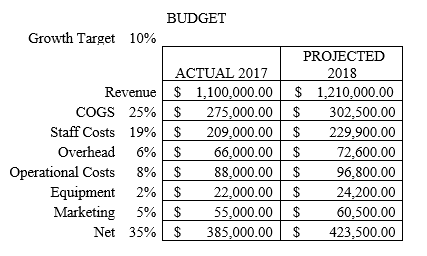 By laying out a budget, and managing it diligently, you will be able to anticipate how much money you can expect to earn this year by making great decisions that adhere to your budget.
By laying out a budget, and managing it diligently, you will be able to anticipate how much money you can expect to earn this year by making great decisions that adhere to your budget.










